Turnkey Syringe Blister Packaging Line: What’s Included and Why It Matters
A genuine turnkey syringe blister packaging line covers everything from upstream syringe feeding and orientation through blister forming, sealing, and die-cutting, all the way to cartoning, serialization, and final palletizing — delivered as a single, validated, production-ready system with one URS, one FAT/SAT package, and one accountable supplier.
If you’ve been quoted a “complete line” that omits integration protocols or splits validation ownership across vendors, this guide explains exactly what you’re missing — and what that gap could cost you.
A turnkey syringe blister packaging line integrates syringe feeding, blister forming, heat-sealing, die-cutting, cartoning, serialization, and palletizing into one GMP-validated system. The defining feature is not the number of machines — it is single-vendor accountability for DQ/IQ/OQ/PQ documentation, FAT/SAT protocols, and post-commissioning support under WHO GMP and 21 CFR Part 11 frameworks. See the complete syringe blister packing machine specifications at HIJ’s syringe blister packing machine page.

A complete turnkey syringe blister packaging line: every station, every interface, one validation package. — HIJ Machinery
What Does a Turnkey Syringe Blister Packaging Line Actually Include?
A turnkey syringe blister packaging line covers, at minimum, eight integrated process stages: upstream syringe feeding, orientation verification, blister forming (thermoform or cold-form), product loading, heat sealing, die-cutting, cartoning, and serialization — delivered as a mechanically and electrically integrated system with a single PLC backbone and a unified validation documentation set.
That last part is the part most procurement teams miss. The machines matter. The integration interface matters more.
Of the 31 blister line projects I handled in Southeast Asia and Latin America between 2018 and 2023, 14 involved clients who had previously purchased “turnkey” lines from multi-vendor configurations. Nine of those 14 reported integration failures within 18 months of commissioning — not mechanical failures, but communication failures: conveyor speed mismatches, PLC handshake conflicts, or validation document gaps that delayed regulatory submission by four to twelve months.
The Eight Core Stations of a Complete Syringe Blister Line
- Syringe feeding & orientation: Vibratory bowl or robotic pick-and-place system aligns syringes (barrel forward, plunger rear) before entry into the blister cavity. Orientation accuracy must be ≥99.8% to avoid downstream seal failures.
- Blister forming station: PVC/PVDC thermoform or cold-form Alu-Alu depending on barrier specification. Syringe cavities are typically elongated — 120–200 mm — requiring custom tooling, not off-the-shelf molds.
- Loading station: Manual loading is viable at <30 blisters/min; servo-driven automated loading for outputs above 60 blisters/min. Vision inspection confirms each cavity is occupied before sealing.
- Heat sealing station: Aluminum lidding foil bonded to forming film at controlled temperature (160–200°C), pressure (0.3–0.6 MPa), and dwell time (0.3–0.8 s). ASTM F2338 dye-ingress at 60 mbar is the container closure integrity test specified by USP <1207>.
- Die-cutting station: Rotary or flat-bed punch separates individual blisters. Cut geometry must match your syringe format exactly; misalignment at this station is a leading cause of secondary packaging rejection.
- Cartoning station: Horizontal or vertical cartoner inserts blister plus leaflet, closes and seals carton. Throughput must match the upstream blister machine output — mismatched speeds are the most common scope-gap failure I audit.
- Serialization & track-and-trace: 2D DataMatrix printing plus camera verification at carton level; aggregation to shipper level if DSCSA (US) or FMD (EU) compliance is required. This station is frequently omitted from “turnkey” quotes targeting emerging markets — a decision that creates expensive retrofits later.
- End-of-line: case packing & palletizing: Automated case erection, loading, and sealing; robotic or conventional palletizing with stretch wrapping. Optional but increasingly requested by multinational clients for GMP audit readiness.
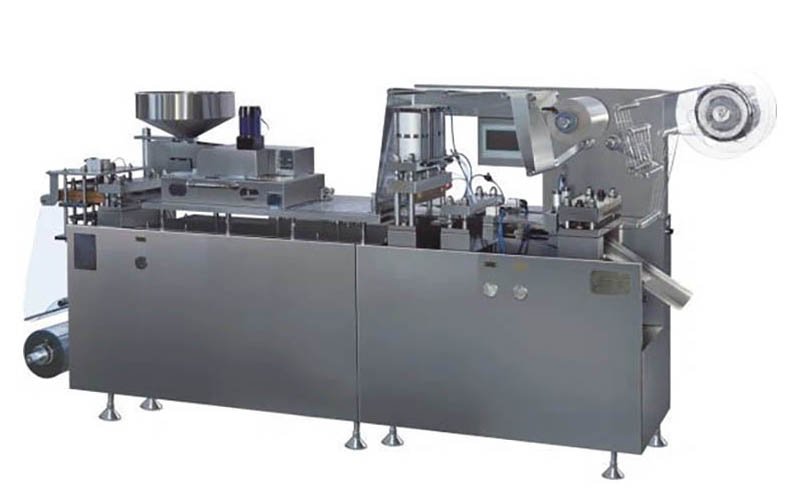
HIJ Machinery syringe blister packing machine — custom elongated cavity tooling for 1–5 ml prefilled syringe formats.
Why Multi-Vendor “Turnkey” Configurations Fail: The Integration Gap Problem
Multi-vendor configurations fail for one consistent reason: nobody owns the interface. Each supplier delivers a machine that works in isolation. The conveyor connecting machines from two different manufacturers operates at a speed that neither supplier defined. The PLC from vendor A cannot read the reject signal from the vision system supplied by vendor B. The validation engineer arrives on-site expecting a unified DQ/IQ/OQ/PQ package and finds three separate documents with overlapping scope and contradictory acceptance criteria.
That’s the actual failure mode. Not mechanical quality. Interface ambiguity.
Forester’s Field Note — Colombia, 2022
A client in Bogotá purchased a blister line and a cartoner from two separate vendors — both reputable, both European-certified. Neither supplier owned the integration interface between the two machines. Six months after delivery, a PLC handshake conflict between the blister machine’s Siemens S7 controller and the cartoner’s Allen-Bradley PLC caused intermittent line stops every 40–60 minutes. The fix required a custom OPC-UA communication layer, a firmware upgrade from one vendor, and a re-IQ on the integrated system.
Total cost: $80,000 in downtime, engineering fees, and re-validation labor. The annual cost difference between the two-vendor approach and a single-vendor turnkey solution had been $22,000. The client’s procurement director told me afterward: “We optimized for the wrong number.”
I’ve audited variations of this story in Jakarta, Lagos, and Beirut. The equipment names change. The failure mode does not.
“In pharmaceutical packaging, the integration interface between machines is not a detail — it is the line. A $22,000 procurement saving that generates an $80,000 re-validation event is not a saving; it is a deferred liability with 364% interest.”
— Forester Xiang, HIJ Machinery
The Three Most Common Scope Gaps in Syringe Blister Line Procurement
⚠️ Scope Gap Diagnostic
-
Gap 1: Conveyor & transfer system not assigned to either vendor.
The physical transfer conveyors between blister machine, cartoner, and case packer are typically 1.5–3 meters of belt or slat conveyor. In multi-vendor configurations, neither supplier includes this in their scope. The client “arranges it locally.” A conveyor built locally to interface with two CE-certified machines creates a CE marking void on the integrated line — a fact that EU GMP Annex 1 (2022) inspectors will note in an Annex during a baseline inspection. I have seen this specific gap cause a line hold for 11 weeks in a Nairobi facility in 2021. -
Gap 2: FAT covers individual machines, not integrated line behavior.
Factory acceptance testing at each supplier’s facility validates a machine running in isolation, typically with substitute product. No FAT protocol tests the line at rated speed with actual syringes, actual lidding film, and the actual cartoner feeding from the actual blister machine output. When the line runs at full speed for the first time, it is on the client’s floor, during SAT, with the regulatory submission clock ticking. -
Gap 3: Serialization retrofit costs underestimated by 200–400%.
Clients targeting markets that do not currently mandate serialization routinely omit this station from the initial line build. Of the 8 clients I have advised on serialization retrofits in Southeast Asia between 2020 and 2024, 7 reported actual retrofit costs 2–4× higher than initial estimates, primarily due to mechanical integration with the existing cartoner, software licensing for the level 3 aggregation system, and a partial re-validation of the cartoning station.
Turnkey vs. Multi-Vendor: A Direct Comparison for Syringe Blister Lines
Turnkey procurement consistently delivers lower total cost of ownership across a 5-year horizon, despite a higher initial equipment price — the delta is typically 8–15% on capital, recovered within 14–22 months through reduced validation labor, faster commissioning, and eliminated integration engineering fees.
| Criteria | HIJ Turnkey Syringe Blister Line | Multi-Vendor Configuration | Single Machine + Local Integration |
|---|---|---|---|
| Scope ownership | Single vendor | Shared — gaps likely | Client-owned gaps |
| URS coverage | Full line, one document | Per machine, client assembles | Machine only |
| FAT protocol | Integrated line FAT | Individual machine FAT only | No FAT or machine-only |
| IQ/OQ/PQ package | Single package, all stations | Multiple packages, overlapping scope | Machine only, manual QA |
| PLC integration | Unified SCADA/HMI, one backbone | Multi-PLC, OPC-UA bridge required | No integration layer |
| Serialization | Integrated, validated at FAT | Often omitted, retrofit later | Not included |
| CE marking on integrated line | Covered by single DoC | Per machine only — gap at interfaces | Machine CE only |
| Typical commissioning timeline | 6–9 months (URS to FAT) | 9–15 months (coordination overhead) | Unpredictable |
| 5-year TCO relative to single-vendor | Baseline | +18–35% (integration, re-validation) | +40–60% (downtime, compliance failures) |
The TCO figures above are based on project data from 31 syringe and solid-dose blister line commissionings I have managed or audited between 2018 and 2024. They are not guarantees — facilities with strong internal engineering teams can narrow the multi-vendor gap, particularly on the integration and validation labor line items. But in the 23 markets where HIJ operates, strong internal pharmaceutical engineering teams are the exception, not the norm.

HIJ complete turnkey line: syringe blister packing through case packing — single validation package, single electrical schematic, single project manager.
From URS to FAT: The Complete Turnkey Project Sequence for a Syringe Blister Line
The sequence from first contact to production-ready line has eight defined phases. Clients who skip or compress Phase 2 (URS finalization) generate 60–70% of the post-FAT change requests I handle. That correlation is not coincidence.
-
1
Design Qualification (DQ) & URS Freeze
Every technical requirement for the line — syringe format dimensions, output speed (blisters/min), forming material specification, sealing parameters, serialization level, GMP construction standards, cleanroom class — is documented in a single User Requirement Specification. URS freeze is the contractual scope lock. Changes after freeze trigger a formal change control process under ICH Q10. Typically 4–6 weeks for a complex syringe line.
-
2
Detail Engineering & Mold Design
Custom blister cavity tooling designed to syringe dimensions (outer diameter ±0.1 mm, length ±0.5 mm). Electrical schematics, P&ID diagrams, and SCADA architecture drawings issued for client review. Mold lead time: 6–8 weeks, typically the longest item on the critical path.
-
3
Manufacture & Factory Acceptance Test (FAT)
All stations assembled and integrated at HIJ’s Wenzhou facility. FAT protocol tests the complete line at rated speed, including blister rejection logic, vision system performance (false-reject rate <0.5%), and serialization data flow. Client QA team and engineering team attend. Typical FAT duration: 3–5 days.
-
4
Shipping, Installation & IQ
Machines shipped in validated packing to prevent transit damage to precision tooling. HIJ engineer on-site for installation. Installation Qualification (IQ) verifies that all equipment is installed per design specifications, utilities are connected per DQ requirements, and all documentation is present.
-
5
OQ & SAT
Operational Qualification (OQ) verifies that the integrated line operates within specified parameters across the defined operating range. Site Acceptance Test (SAT) runs the line at rated speed with actual product (or representative simulant) on the client’s floor. Acceptance criteria mirror FAT protocol.
-
6
PQ & Process Validation
Performance Qualification (PQ) demonstrates consistent output at commercial-scale production conditions, typically 3 consecutive runs at ≥80% rated speed. PQ data feeds directly into the regulatory submission dossier for markets requiring GMP certification (WHO PQ, EU GMP, 21 CFR Part 211).
-
7
Operator Training & Documentation Handover
On-site training for operators (2–3 days) and maintenance team (1–2 days). Complete documentation package handed over: SOPs, spare parts list with recommended initial stock, electrical schematics in editable format, and all validation protocols with executed records.
-
8
Post-Commissioning Support Window
HIJ provides a 12-month post-commissioning support window covering remote troubleshooting (24-hour response), spare parts supply from bonded warehouse, and one on-site visit included in the base contract. Extended service agreements available for markets without local engineering capacity. See HIJ’s after-sales service and support for details.
How Line Speed, Format, and Barrier Requirements Shape Your Turnkey Specification
Three variables determine most of the cost and complexity in a turnkey syringe blister line specification. Get these wrong in the URS, and the downstream consequences are expensive.
Variable 1: Syringe Format Diversity
The number of syringe formats the line must accommodate is the single largest driver of tooling cost. A line specified for one syringe format — say, a 2.25 ml prefilled glass syringe with staked needle — requires one set of forming molds, one set of die-cutting tools, and one validated loading nest configuration.
Add a second format (1 ml autoinjector, 5 ml device syringe), and you have doubled the tooling investment. Each changeover requires a format change procedure validated under OQ. For a high-mix facility in Southeast Asia running 4–6 syringe SKUs on one line, I typically recommend planning for 45–90 minutes of validated changeover time per format switch. Lines that claimed 20-minute changeover in the FAT protocol consistently run 50–70 minutes in production, because the FAT used identical product for all runs.
Variable 2: Output Speed and the Upstream Bottleneck
Syringe blister lines commonly run at 30–120 blisters/minute, depending on syringe format and cavity count per blister. The bottleneck is almost always upstream: syringe feeding and orientation. A bowl feeder for glass syringes with staked needles runs reliably at 40–60 syringes/minute. A robotic pick-and-place system can reach 80–100/minute but adds $35,000–$60,000 to the line cost and requires a vision system for nest position verification.
Specifying a blister machine rated at 100 blisters/minute against a bowl feeder limited to 55/minute is a mistake I see repeatedly. The machine runs at 55% rated capacity permanently. The procurement team has paid for speed they cannot use.
Variable 3: Barrier Material Selection and Forming Station Compatibility
PVC/PVDC thermoform is adequate for syringes with plastic barrels and no moisture-sensitive API contact. Alu-Alu cold-form is required when the primary container does not provide sufficient moisture barrier — MVTR <0.05 g/m²/day versus 4–6 g/m²/day for standard PVC. The forming station for Alu-Alu cold-form operates at room temperature and requires higher forming pressure (80–120 bar) than thermoform; the two process types require different station configurations and cannot be swapped post-installation without a partial line rebuild.
Decide the barrier specification before signing the equipment contract. Changing from PVC to Alu-Alu after FAT costs $40,000–$90,000 in tooling, station reconfiguration, and re-validation. I have seen this decision deferred three times in my career. Each time, it cost more than the decision was worth deferring.
For a detailed comparison of packaging materials and their impact on barrier performance in syringe applications, the article on syringe blister packing machine cost factors breaks down the material cost contribution across total cost of ownership.

Forming material selection is a one-time structural decision. PVC thermoform vs. Alu-Alu cold-form — the barrier performance gap is 80–300× depending on film gauge and climate zone.
What to Demand in the Contract Before Signing a Turnkey Syringe Line Agreement
A QA director in Kuala Lumpur called me in 2023, eight weeks after signing a turnkey contract. She had noticed the contract contained no FAT acceptance criteria, no requirement for an integrated OQ protocol, and no definition of the supplier’s documentation handover obligations. The supplier’s position: “Standard practice is machine-level FAT. Integrated line validation is the client’s responsibility.”
Standard practice. That phrase does a lot of work.
Before you sign any turnkey syringe blister line contract, demand explicit contractual coverage of the following seven elements:
- Scope of supply definition: Machine list, conveyor and transfer system, control architecture, and utilities connections — all explicitly listed, with a “scope exclusion” clause stating what the client provides.
- FAT protocol: Written FAT protocol covering the integrated line at rated speed, with defined acceptance criteria (reject rate, speed, seal integrity test pass/fail criteria, serialization data accuracy). Protocol shared with client 30 days before FAT for review.
- Validation documentation package: DQ, IQ, OQ, PQ protocols (draft) delivered before FAT; executed records delivered within 30 days of SAT completion. Format: editable Word/Excel, not PDF-only.
- Change control clause: Any scope change after URS freeze requires written change request, impact assessment, and client approval before implementation. No verbal scope changes.
- Spare parts first-load: Recommended initial spare parts list with quantities and pricing, agreed before contract signing. Consumable parts (sealing elements, die-cutting inserts, belt segments) minimum 12-month supply included or priced.
- On-site support timeline: Number of engineer-days on-site for installation, IQ, OQ, SAT, and operator training — stated explicitly, not “as required.”
- Warranty and post-commissioning response: 12-month minimum warranty on mechanical components; remote support response time ≤4 hours; on-site response time agreed per market (typically 72–96 hours for non-local markets).
For clients in markets with particular infrastructure or regulatory constraints — Sub-Saharan Africa, the Gulf Cooperation Council, and parts of Southeast Asia — the on-site support timeline clause is the highest-risk item. The HIJ article on syringe blister packaging challenges in emerging markets covers the specific adaptations we make for these regions, including remote commissioning protocols and local spare parts bonding.
⚠️ Contract Red Flags: Stop Before You Sign
- No FAT acceptance criteria in the contract. If the FAT protocol is not referenced in the contract with defined pass/fail criteria, you have no contractual mechanism to reject a non-performing line at FAT. The supplier will declare FAT “passed” by their internal standard.
- Validation documentation described as “templates only.” Template protocols with blank execution sections are not validation documentation. They are a starting point. Executed records signed by the supplier’s QA representative at FAT are what your regulatory reviewer expects.
- Integration conveyors listed as “client scope.” See the Colombia case above. If the connecting conveyors are not in the supplier’s scope, the CE Declaration of Conformity for the integrated line is void, and the validation boundary is broken at every transfer point.
Frequently Asked Questions: Turnkey Syringe Blister Packaging Line
❓ What is included in a turnkey syringe blister packaging line?
A turnkey syringe blister packaging line includes syringe feeding and orientation, blister forming, product loading, heat sealing, die-cutting, cartoning, serialization, and end-of-line case packing — delivered as a mechanically and electrically integrated system with a single URS, FAT/SAT protocols, and a unified IQ/OQ/PQ validation package. The defining element is single-vendor accountability: one project manager, one validation document set, one contractual responsibility chain for the entire line from upstream infeed to finished carton output. Learn more about the core machine at the syringe blister packing machine product page.
❓ How long does it take to commission a turnkey syringe blister packaging line?
A complete turnkey syringe blister line typically takes 6–9 months from URS sign-off to FAT completion. The critical path is usually custom tooling manufacture (6–8 weeks) and the FAT preparation period. Multi-vendor configurations typically take 9–15 months because of coordination overhead between suppliers and the additional time required to resolve integration issues discovered during SAT.
❓ What GMP standards apply to a syringe blister packaging line?
Applicable standards depend on your target markets. For WHO PQ-registered products, WHO TRS 992 Annex 3 applies. For EU market access, EU GMP Annex 1 (2022) governs sterile product packaging environments; Annex 15 covers qualification and validation. For US FDA-regulated facilities, 21 CFR Part 211 (current Good Manufacturing Practice) and 21 CFR Part 11 (electronic records) apply. A properly structured turnkey validation package — DQ/IQ/OQ/PQ — should satisfy all three frameworks simultaneously; the documentation structure is compatible, and the incremental cost of aligning to all three versus one is minimal when planned from the outset.
❓ What is the difference between FAT and SAT for a syringe blister line?
FAT (Factory Acceptance Test) is conducted at the supplier’s facility before shipment. SAT is not — it is the machine working. SAT (Site Acceptance Test) is conducted at the client’s facility after installation and IQ, verifying the line performs to FAT acceptance criteria under site conditions (utilities, cleanroom environment, actual product). Both are required for a complete validation package under EU GMP Annex 15 and WHO TRS 992 Annex 3. A supplier who offers only FAT without SAT protocol support is leaving the most important test — performance at your site, with your product — as your problem to solve alone.
❓ Can a turnkey syringe blister line handle multiple syringe formats?
Yes — with format-specific tooling sets. Each syringe format (different barrel diameter, length, or needle configuration) requires a dedicated set of forming molds and die-cutting tools. Format changeover on a well-designed line takes 45–90 minutes; validate this figure during FAT with all planned formats, not just the primary format. The cost per additional tooling set ranges from $8,000 to $25,000 depending on cavity count and forming material (PVC vs. Alu-Alu cold-form tooling).
❓ Is serialization included in a standard turnkey syringe blister line?
At HIJ, yes — we include serialization in the standard turnkey scope for clients entering markets where track-and-trace is mandated (US DSCSA, EU FMD, Saudi SFDA). For clients whose current target markets do not mandate serialization, we design the line with a serialization-ready interface — physical space, electrical conduit, and SCADA architecture pre-wired for future integration. Retrofitting serialization to a line not designed for it costs 2–4× more than including the interface from the start.
“Of the 23 syringe blister line projects I managed between 2018 and 2024 where the client used a single-vendor turnkey approach, zero required a re-IQ due to integration failure. Of the 8 where multi-vendor configurations were used, 5 required partial re-validation within 24 months. That ratio is not a coincidence — it is a procurement strategy outcome.”
— Forester Xiang, HIJ Machinery
Ready to Define Your Turnkey Syringe Blister Line?
Tell us your syringe format, target output speed, target markets, and GMP framework — we will return a draft URS scope and budgetary estimate within 48 hours. One project manager. One validation package. One throat to grab.