📦 Packaging Format Decision Guide
Blister Packaging vs Bottle Filling for Pills: A Decision That Will Lock In Your Production Line for a Decade
The choice between blister packaging and bottle filling is not about which looks better on the shelf. It is a regulatory, stability, and total-cost-of-ownership decision — and I have watched mid-sized manufacturers get it wrong in ways that cost them years of re-validation and hundreds of thousands in retrofit fees.
This guide maps both formats across every decision variable that matters: moisture barrier performance, GMP compliance burden, unit economics, market fit, and the regulatory channels your product actually needs to enter. Map your URS against these criteria before you sign any equipment purchase order.
⚡ Direct Answer
Blister packaging suits moisture-sensitive oral solid dosage forms, unit-dose regulatory markets (EU, hospital tenders), and products with controlled dosing requirements. Bottle filling is better for high-volume OTC solids, bulk dispensing markets, and lines where low CAPEX and fast format changeover dominate the decision. Neither format is universally superior — the right answer depends on your API stability profile, target market, and validated throughput requirements. For a full specification walkthrough of a pill blister packaging machine, start with the technical detail on the DPP-260 product page.

Blister packs vs HDPE bottles: the format decision determines your regulatory pathway, stability data requirements, and line investment for years ahead.
What Makes the Blister vs Bottle Decision Genuinely Difficult — and Why Most Buyers Get It Wrong
The number teams look at first is exactly the wrong number. CAPEX.
A standard HDPE bottle filling line for oral solid dosage forms runs $80,000–$200,000 for a mid-speed system. A flat-die pill blister packaging machine with comparable throughput — 40,000–60,000 tablets per hour — sits in the $90,000–$250,000 range depending on forming material capability and automation level. The CAPEX delta looks manageable. The problem emerges 18 months later, when your stability batch fails at Zone IVb conditions (40°C/75% RH) and your product was packaged in a 200ml HDPE bottle with a CRC cap.
I have seen this exact scenario play out three times in Southeast Asian markets between 2019 and 2023. Each time, the manufacturer had generated stability data under Zone II conditions (25°C/60% RH) because that matched their local climate at the time of dossier submission. Each time, the distribution footprint expanded to a tropical region after commercialization. And each time, the retrofit cost — new line, new IQ/OQ/PQ validation, new dossier variation filing — ran between $380,000 and $1.2 million.
The CAPEX number on the first quotation looks very different by then.
📋 What this guide covers
This comparison covers moisture barrier performance, GMP compliance requirements, per-unit economics, market channel fit, and the specific API profiles where each format is the correct — or wrong — choice. If you are still mapping the basics of what a blister packaging machine is, that foundation article is a useful starting point before going deeper into this format comparison.
Moisture Vapor Transmission: The Number That Determines Which Format Wins for Your API
Blister packaging — specifically Alu-Alu cold-form format — cuts moisture vapor transmission to 0.02–0.5 g/m²/day, compared to 4–6 g/m²/day for standard PVC thermoform and 15–35 g/m²/day for a 200ml HDPE bottle at 40°C/75% RH. That is a 30x to 1,750x difference in barrier performance, and it is the central technical fact that should drive your format decision before you look at anything else.
For a hygroscopic API with 0.5% w/w moisture uptake threshold at 75% RH — the kind that shows up routinely on tropical market formularies — that barrier gap is the difference between an 18-month shelf life and a 6-month shelf life. Wrong format. Your product degrades on the shelf. Your batch recall follows.
Moisture Barrier by Packaging Format — Pharmaceutical Reference Data
| Packaging Format | MVTR (g/m²/day at 40°C/75% RH) | Typical Shelf Life Achievable | Best Fit API Profile | Regulatory Markets |
|---|---|---|---|---|
| Alu-Alu Cold-Form Blister | 0.02 – 0.5 | 24–36 months (tropical) | Highly hygroscopic, light-sensitive, oxygen-sensitive APIs | EU, US, WHO prequalified markets |
| PVC/Alu Thermoform Blister | 4 – 6 | 18–24 months (temperate) | Moderate moisture sensitivity, standard oral solids | Southeast Asia OTC, LATAM, India |
| PVDC/Alu Thermoform Blister | 0.5 – 2 | 24 months (tropical) | Moderate-high moisture sensitivity, budget-constrained Alu-Alu alternative | Broad emerging markets |
| HDPE Bottle (200ml, CRC cap) | 15 – 35 | 18–24 months (temperate only) | Low moisture sensitivity, stable APIs, OTC vitamins | US OTC, UK OTC, mass retail |
| Glass Bottle (Type III) | Near zero (inorganic barrier) | 36–60 months | Highly reactive or light-sensitive APIs; premium/injectable adjacent | EU hospital, US Rx premium |
The PVDC row is important. It is the middle path many manufacturers in Southeast Asia and LATAM choose when cold-form Alu-Alu feels cost-prohibitive but standard PVC fails Zone IVb stability. PVDC barrier at 0.5–2 g/m²/day handles most tropical market dossiers without triggering a full line equipment change — the forming station on a PVC-capable machine usually handles PVDC with a forming temperature adjustment.
The MVTR number is the first thing I ask for when a client tells me they cannot decide between blister and bottle. If their API absorbs more than 0.3% w/w moisture at 75% RH and their target market sits in ICH Zone III or IVb, the conversation about bottles is over in about four minutes. — Forester Xiang, HIJ Machinery

Unit-dose blister packs provide per-cavity moisture isolation — a barrier architecture that HDPE bottles fundamentally cannot replicate once the container is opened.
GMP Compliance Requirements: Where Blister Lines and Bottle Lines Differ in Validation Burden
Both formats require IQ, OQ, and PQ validation under EU GMP Annex 15 and 21 CFR Part 211.68. The practical difference is where the validation risk concentrates.
A CDSCO reviewer cited ICH Q1A(R2) directly in a 2022 dossier review I was supporting for a client expanding from India into Nigeria. The question was not whether their blister line was validated — it was. The question was whether the sealing integrity data covered 40°C/75% RH storage conditions continuously across a 12-month accelerated window. The dossier had Zone II data. It went back. Eight months later, it came back with a Zone IVb package. By then, the launch window for the tender cycle had closed.
For bottle lines, the equivalent failure mode is container closure integrity (CCI) testing. USP <1207> requires CCI verification for all primary packaging systems — and HDPE bottle lines running 300+ bottles per minute generate enormous variation in cap torque consistency. The 21 CFR Part 211.94 requirement for component qualification means every desiccant cap lot, every induction seal lot, every bottle dimensional batch needs incoming QC documentation. That cost is invisible on the equipment price quotation.
✅ Compliance Reference Snapshot
Sealing integrity validation for blister lines: ASTM F2338 (dye ingress at 60 mbar), as specified in USP <1207>. Bottle CCI: USP <1207.1> (deterministic) or USP <1207.2> (probabilistic). Both formats fall under EU GMP Annex 15 qualification requirements and WHO TRS 992 Annex 3 for WHO-prequalified markets.
One data point worth anchoring: FDA enforcement records for 2019–2023 identify packaging as the root cause in approximately 12% of pharmaceutical recalls — the category with the strongest correlation to tropical market distribution failures. The majority of those cases involve inadequate barrier specification in the original packaging design, not equipment malfunction on the line.
Market Channel Fit: Where Each Format Wins Without Argument
A QA director in São Paulo called me last year. Her company had just lost a Ministry of Health hospital tender — not on price, not on dossier quality. On packaging format. The tender specification required unit-dose blister presentation. Her line ran bottles. Fourteen months of tender preparation, gone.
This is not an edge case. It is structural.
Channels Where Blister Packaging Wins
- EU hospital and reimbursement tenders: Unit-dose blister is the default format specification. Hospitals require per-dose dispensing accountability under EU Directive 2011/62/EU (falsified medicines) and local tender terms.
- WHO prequalification programs: WHO TRS 992 Annex 3 guidance for tropical markets (Zone IVb) strongly correlates with blister or Alu-Alu primary packaging for moisture-sensitive APIs.
- Prescription Rx markets with strict dose tracking: Unit-dose serialization (as required by EU FMD and 21 CFR Part 211 serialization guidelines) is mechanically simpler on blister lines, where each card is a discrete, scannable unit.
- Products with pediatric tamper-evidence requirements: Push-through blister packs with child-resistant peel-push film (ISO 8317 compliant) are harder to defeat than CRC caps for pediatric populations.
- High-value branded Rx with anti-counterfeiting needs: Blister card serialization, holographic foil lidding, and track-and-trace at the unit-dose level are all more accessible in blister format than in bulk bottle lines.
Channels Where Bottle Filling Wins
- High-volume OTC vitamins and supplements: 90-count and 120-count HDPE bottles dominate US, UK, and Australian mass-market retail. Consumer familiarity and low per-unit dispensing cost drive the channel.
- Products with variable dose regimens: When the prescribing physician adjusts dose mid-course, a 30-count or 60-count bottle allows pharmacy dispensing flexibility that blister cards cannot match without a line changeover.
- Lines requiring format agility across count sizes: Bottle lines switch from 30-count to 90-count with a turret change and count wheel adjustment — typically under 30 minutes. Blister lines changing card format (8-cavity to 10-cavity) require a full tooling changeover: forming die, sealing die, cutting die. Typically 2–4 hours.
- Bulk dispensing pharmacy markets: Canada, Australia, and parts of the US still operate bulk-dispensing pharmacy models where bottles are the only format that pharmacists will accept for repackaging.

Blister, strip pack, and bottle filling lines each occupy distinct positions in the pharmaceutical packaging equipment landscape — the right format is determined by API profile and market channel, not CAPEX alone.
Unit Economics: What Each Format Actually Costs at Scale — Including the Variables Nobody Quotes You Up Front
Of the 31 blister line projects I handled in Southeast Asia and LATAM between 2018 and 2023, 14 involved clients who had originally built business cases around bottle lines. In 9 of those 14 cases, the per-unit cost advantage of bottles evaporated within 24 months — not because the equipment failed, but because material and compliance costs were never fully modeled in the original business case.
Here is the real cost structure.
| Cost Variable | Blister Packaging Line | Bottle Filling Line | Notes |
|---|---|---|---|
| Equipment CAPEX (mid-speed) | $90,000 – $250,000 | $80,000 – $200,000 | Blister range widens significantly with Alu-Alu forming capability |
| Tooling (per format change) | $8,000 – $25,000 per mold set | $1,500 – $6,000 per turret set | Blister tooling cost is a real differentiator for multi-SKU operations |
| Primary packaging material (per 1,000 units) | PVC/Alu: $0.80 – $1.40 Alu-Alu: $2.20 – $4.50 |
HDPE bottle + cap + desiccant: $0.55 – $1.20 | Bottle appears cheaper; desiccant cost is often omitted from initial quotes |
| IQ/OQ/PQ validation (initial) | $45,000 – $120,000 | $35,000 – $90,000 | CCI testing adds $15,000–$40,000 to bottle line validation for regulated markets |
| Changeover time (format) | 2 – 4 hours (full mold change) | 20 – 40 minutes (turret swap) | Blister changeover OEE impact is significant at <3 SKUs per line |
| Regulatory re-submission (format change after approval) | Type II variation (EU): $50,000–$200,000 + 12–18 months | Same if changing from blister to bottle post-approval | This is the hidden cost nobody models at year zero |
| Waste / reject rate at steady state | 0.3% – 1.2% (forming + sealing defects) | 0.1% – 0.5% (underfill, cap seal) | Blister reject rates improve significantly with servo-driven forming systems |
The procurement director at a mid-sized generics manufacturer in Malaysia once showed me his cost sheet. Bottles: $0.006 cheaper per unit than blister at their 8-million-unit annual volume. Total annual saving: $48,000. I asked what a batch recall cost. He knew the number. He did not say it out loud. They moved to blister that year.
For a deeper look at how equipment investment breaks down across the full cost lifecycle, the blister packaging machine cost breakdown guide covers total cost of ownership in detail — including tooling, validation, and material cost modeling across 3-year production horizons.
⚠️ Decision Traps: Where Manufacturers Choose Wrong and Why
🔴 Trap A: Choosing bottle because CAPEX is $30,000 lower
What happens: Zone IVb stability data fails at 12-month accelerated point. Product’s moisture uptake at 75% RH exceeds the API degradation threshold. The API was documented as “low hygroscopicity” in the formulation file — but that classification was made at 25°C, not 40°C.
The actual cost: Type II variation filing in target market + new stability package + re-validation of blister line. Typical total: $280,000–$600,000 and 14–22 months of delay.
🔴 Trap B: Choosing blister for an OTC product going to bulk-dispensing markets
What happens: Retail buyers in target market (e.g., Canada, Australia) request bottle presentation because pharmacists repackage from bulk. Blister format cannot be sold into that channel without a format variation filing.
The fix at year zero: Confirm distribution channel format requirements with three distributors in the target market before writing the URS. Add 6 weeks to the project timeline. Save 18 months of retrofit.
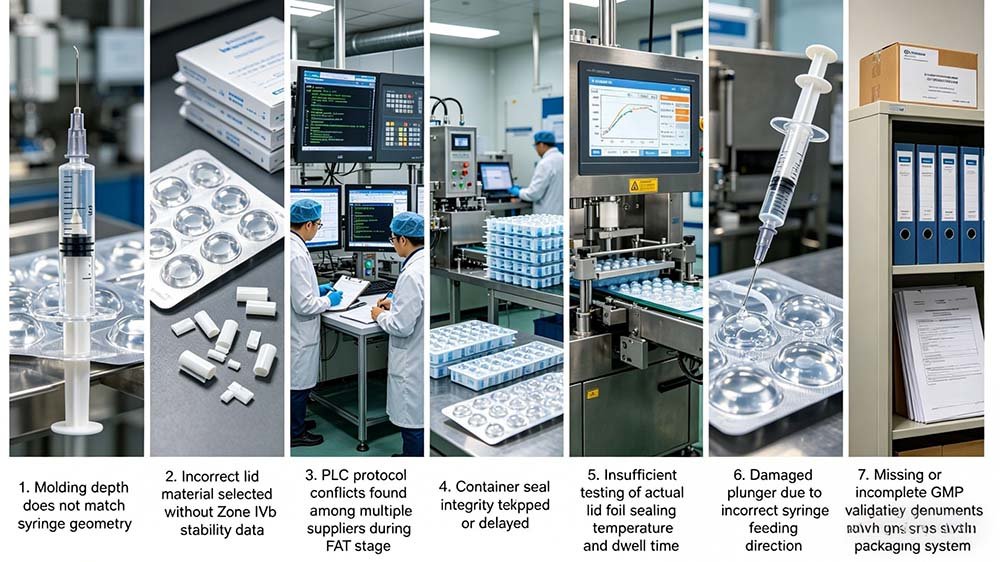
🔴 Trap C: Assuming validated blister documentation from a budget supplier is audit-ready
What happens: The machine arrives with a validation folder. The IQ protocol references internal test methods not traceable to pharmacopoeial standards. The FDA inspector or EU GMP auditor asks for the calibration records of the sealing station thermocouples. They do not exist in the supplied documentation.
The fix: Before purchase, request the actual IQ/OQ template used for a comparable previously delivered machine. Ask specifically for thermocouple calibration traceability records and ASTM F2338 sealing integrity test data. A supplier that has done this before will produce these documents in under 24 hours.
The Decision Framework: A Four-Variable Filter That Works for 90% of Pharmaceutical Packaging Decisions
I will not tell you this decision is simple. It involves your API stability profile, your target market regulatory framework, your validated throughput requirement, and your five-year product portfolio plan. But in 20 years, four variables have separated blister-right from bottle-right decisions in every market I have worked in — Southeast Asia, LATAM, the Middle East, Sub-Saharan Africa.
🎯 Four-Variable Format Decision Filter
- ✅API moisture uptake >0.3% w/w at 75% RH (Zone III/IVb markets)
- ✅Target channel: EU hospital tenders, WHO prequalified, Rx unit-dose
- ✅Serialization / track-and-trace at unit-dose level required (EU FMD, DSCSA)
- ✅Product portfolio is <5 SKUs per line (changeover frequency manageable)
- ✅Light-sensitive or oxygen-sensitive API requires barrier beyond HDPE
- ✅API is stable at 40°C/75% RH through 18-month window in HDPE
- ✅Target channel: US/UK/AU mass OTC retail, bulk pharmacy dispensing
- ✅Variable dose regimen requires pharmacist-level dispensing flexibility
- ✅>8 SKUs per line with frequent count changes (turret swap faster than mold change)
- ✅High-volume, price-sensitive generics where per-unit material cost is the margin
There is a fifth variable that overrides all four. Regulatory precedent. If your reference market dossier was approved with blister packaging, changing to bottles after approval requires a Type II variation in EU or a Prior Approval Supplement in the US. That is a 12–24 month process with associated consulting, stability, and filing fees. Do not build a business case around a packaging format you plan to change post-approval. The cost is never worth it.

A GMP-compliant blister packaging line running unit-dose pharmaceutical products — the format of choice for EU hospital tenders, WHO prequalified markets, and moisture-sensitive APIs.
A 20-Year Engineer’s Perspective: The Question Nobody Asks Until It Is Too Late
🧑 Forester’s Insight: Field Experience
The choice between blister packaging and bottle filling is not purely about aesthetics — it is a regulatory, stability, and total-cost-of-ownership decision that will shape your production line investment for the next decade. In 20 years of auditing pharma facilities across Southeast Asia and LATAM, I have watched mid-sized manufacturers lock themselves into the wrong format by choosing bottle lines for moisture-sensitive tablets simply because the CAPEX looked lower on paper. The trap nobody mentions: when your product fails stability testing 18 months later, the retrofit cost and regulatory re-submission fees dwarf the original “savings.”
Before committing to either format, map your URS against your target market’s regulatory demands. Unit-dose blister lines dominate EU and hospital-tender channels. HDPE bottle lines suit high-volume OTC markets. At HIJ, we guide clients through this decision as part of our turnkey integration philosophy — ensuring the chosen line is validated, compliant, and audit-ready from day one. Explore how that works on the DPP-260 pill blister packaging machine page, or review your selection criteria against the full blister packaging machine selection guide.
The question nobody asks at the specification stage: “What does my distribution network look like in five years, and does my packaging format need to change to access new channels?” I have had that conversation after equipment installation. It is a much worse time to have it than before the purchase order is signed.
$2.3 million. That is what one manufacturer I worked with in Indonesia spent on a packaging format retrofit and re-dossier exercise between 2020 and 2022 — moving from bottle to blister for a product targeting WHO prequalification. The original blister line they declined to buy in 2019 was quoted at $140,000.
Frequently Asked Questions: Blister Packaging vs Bottle Filling for Pharmaceutical Pills
❓ Is blister packaging always better than bottle filling for pharmaceutical tablets?
No. Blister packaging is better for moisture-sensitive APIs, unit-dose regulatory markets, and products requiring per-dose serialization. Bottle filling is better for high-volume OTC products distributed through bulk-dispensing pharmacy channels, and for products with variable dose regimens where pharmacist repackaging flexibility matters. Neither format is universally superior — the correct choice depends on your API stability profile, target market regulatory channel, and five-year portfolio plan.
❓ Which packaging format does the EU require for hospital tenders?
EU hospital and reimbursement tenders overwhelmingly specify unit-dose blister presentation. This is not a formal legal requirement in most EU member states, but tender specifications consistently mandate per-dose dispensing format — which blister packs satisfy and bulk bottles do not. Under EU Directive 2011/62/EU (falsified medicines framework), individual unit serialization is also required, and blister cards provide a more straightforward serialization architecture than bottle labels.
❓ How much does it cost to switch from bottle to blister packaging after regulatory approval?
Switching primary packaging format after regulatory approval requires a Type II variation in EU (typically $50,000–$200,000 in fees, stability studies, and dossier preparation, plus 12–18 months timeline) or a Prior Approval Supplement in the US FDA pathway. Total cost including new line equipment, IQ/OQ/PQ validation, and regulatory filing typically runs $280,000–$1.2 million depending on the market and product complexity. This is the core reason the format decision must be made at URS stage, not after commercialization.
❓ What is the moisture vapor transmission rate difference between blister and bottle packaging?
Alu-Alu cold-form blister delivers 0.02–0.5 g/m²/day MVTR at 40°C/75% RH. Standard PVC thermoform blister: 4–6 g/m²/day. A 200ml HDPE bottle with CRC cap: 15–35 g/m²/day. For a hygroscopic API with a 0.3% w/w moisture uptake limit, only cold-form Alu-Alu blister reliably maintains product stability in ICH Zone IVb tropical markets across a 24-month shelf life window.
❓ Can the same pharmaceutical production line run both blister and bottle formats?
No. Blister and bottle filling are mechanically incompatible — they are separate equipment categories. A blister line forms, fills, seals, and cuts individual push-through cards. A bottle filling line fills, caps, labels, and conveys containers. Manufacturers operating both formats require two separate validated lines, each with its own IQ/OQ/PQ documentation. Some high-volume operations run parallel lines for different SKU segments: blister for Rx and tender markets, bottles for OTC retail.
❓ Which format has a lower per-unit packaging material cost?
Bottle filling has lower per-unit material cost for standard OTC volumes — approximately $0.55–$1.20 per 1,000 units (HDPE bottle + CRC cap + desiccant) versus $0.80–$1.40 per 1,000 units for PVC/Alu blister. However, this comparison changes significantly when desiccant cost, induction seal lot qualification, and container closure integrity testing are fully included in the bottle-side cost model. Alu-Alu blister material at $2.20–$4.50 per 1,000 units is higher, but the regulatory and stability risk reduction it provides in tropical markets typically justifies the premium.
❓ How long does format changeover take on a blister line versus a bottle line?
Blister line format changeover — changing from one cavity configuration to another — requires replacing the forming die, sealing die, and cutting die. Typical changeover time: 2–4 hours with a trained operator. Bottle line format changeover (count size or container size) typically involves a turret or counting disc swap: 20–40 minutes. This OEE difference is meaningful for operations running more than 5 SKUs per line and makes bottle lines more agile for multi-SKU OTC portfolios.
❓ What pill sizes can a blister packaging machine handle?
Most pharmaceutical-grade blister machines handle tablets from 3mm to 22mm diameter and capsules from size 00 to size 5, including oval, oblong, and non-standard shaped forms. Cavity geometry is defined by the forming mold — any product outside standard dimensions requires a custom mold design, typically adding $8,000–$15,000 to the tooling budget and 4–8 weeks to the project timeline.
Ready to Confirm the Right Format for Your Product and Market?
The format decision is the most consequential equipment choice in your packaging project. Before you write the URS, map your API stability data, target regulatory channel, and five-year SKU plan against these criteria with someone who has commissioned lines in the markets you are entering. HIJ Machinery guides clients through this decision as part of our turnkey line philosophy — no format lock-in without dossier-ready validation documentation to back it up.