Vacuum filling evacuates air from the syringe barrel during both filling and stoppering, eliminating entrapped bubbles and headspace oxygen. Standard (atmospheric) filling dispenses at ambient pressure and is faster and cheaper. For pharmaceutical manufacturers, the deciding factor is product viscosity and oxygen sensitivity: aqueous, oxygen-stable formulations run fine on standard fillers, while viscous gels and biologics require vacuum filling to avoid batch rejection.
Rule of thumb: above roughly 1,000 cP, or with any oxygen-sensitive API, specify vacuum.
The procurement verdict: vacuum capability adds cost to the machine but removes a recurring, compounding cost — rejected syringes and failed batches. If your product is viscous or oxygen-sensitive, the payback period is usually measured in batches, not years.
This comparison is written for pharmaceutical manufacturers, contract fillers (CDMOs) and plant engineering teams specifying a prefilled syringe line. It assumes you are evaluating capital equipment against a defined formulation, batch size and validation timeline — not browsing consumer products. If you are new to the equipment category, start with our overview of what a prefilled syringe filling machine is.
Vacuum filling vs. standard filling: head-to-head
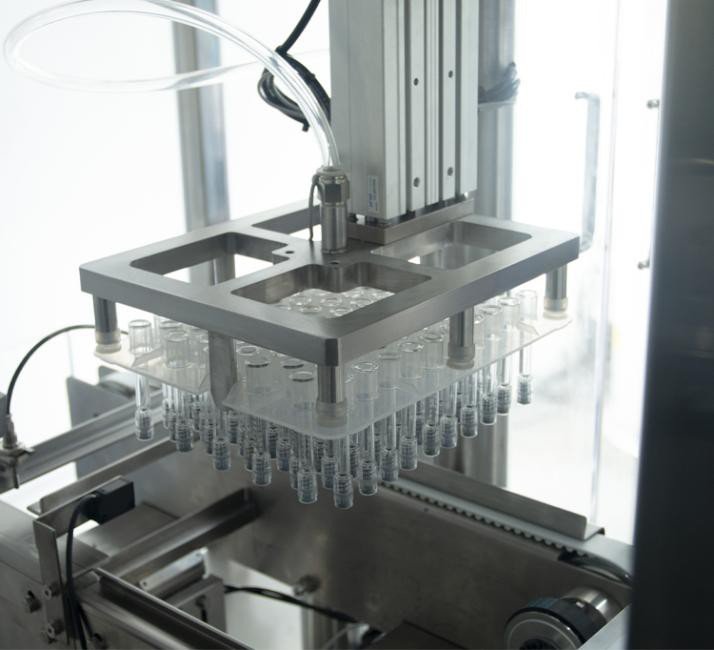
Both methods use a metering pump to dispense a fixed dose into a pre-sterilized (SCF/RTF) syringe. The difference is the pressure environment inside the barrel during the fill and stoppering strokes — two distinct stations, each running under vacuum on a vacuum-type machine.

| Criterion | Vacuum filling | Standard (atmospheric) filling |
|---|---|---|
| Air entrapment | Eliminated — barrel evacuated before & during fill | Likely on viscous product |
| Headspace oxygen | Minimised — stoppered under vacuum | Ambient air sealed in |
| Stopper rebound (“pop-up”) | Prevented — vacuum holds stopper on liquid | Possible with trapped air |
| Suitable viscosity | Low to very high (gels, ointments, >20,000 cP) | Low (aqueous, water-like) |
| Typical throughput | Lower — vacuum dwell adds cycle time | Higher — no dwell |
| Equipment CAPEX | Higher (vacuum system + controls) | Lower |
| Rejection risk (viscous API) | Low | High |
| Best fit | Biologics, mAbs, HA/dermal fillers, ophthalmic gels | Saline, aqueous vaccines, simple solutions |
Why bubbles are a commercial problem, not just a cosmetic one

For a plant manager, an air bubble is not an aesthetic defect. It is a documented deviation. A visible bubble in a prefilled syringe can affect deliverable dose accuracy, trigger a visual-inspection reject, and — if the rate is high enough — put the batch record under investigation. On oxygen-sensitive biologics, entrapped headspace oxygen also drives oxidative degradation that shortens shelf life.
Worked example: the cost of a 3% reject rate
Illustrative model only — substitute your own batch size, reject rate and loaded cost. The point is directional: on a viscous product, scrap cost dominates the equipment premium.
That arithmetic is why we publish the machine price openly rather than hiding it. A base prefilled syringe vacuum filling machine starts at US$26,000 FOB; the full cost breakdown is in our price guide. Against the scrap figures above, the capital delta is rarely the deciding number.
Evaluating a viscous or oxygen-sensitive formulation? Send us the viscosity and syringe format — we will tell you honestly whether you need vacuum.
Request a Formulation ReviewWhen standard filling is the right specification
Vacuum is not universally required, and over-specifying wastes capital and cycle time. Standard atmospheric filling remains the correct choice when:
- The product is low-viscosity and aqueous — saline, many vaccines, simple small-molecule solutions.
- The API is not oxygen-sensitive and headspace oxygen has no stability impact.
- Throughput is the binding constraint and validation data shows no bubble-related rejects.
- You are filling plastic syringes for diagnostics or devices — see our prefilled plastic syringe filling machine.
If throughput on a viscous product is the constraint, the answer is usually not to abandon vacuum but to add filling needles — a double-head vacuum filler keeps the vacuum cycle while lifting output to 800–1,200 syringes/hour (a ~1.5× gain, not a true doubling — vacuum dwell time doesn’t halve).
Key Takeaways for Specifiers
- Viscosity and oxygen sensitivity decide the method — not throughput and not budget.
- Vacuum removes entrapped air and prevents stopper rebound; both are reject drivers.
- On viscous product, scrap cost outweighs the CAPEX premium, often within one or two batches.
- Standard filling is correct for aqueous, oxygen-stable formulations — don’t over-specify.
- Need vacuum and speed? Add needles (double-head), don’t drop the vacuum cycle.
- Always validate on your own formulation at FAT — a water demo proves nothing.

Forester Xiang
Founder & Chief Engineer · 20+ years in sterile filling
Every filling machine on earth looks perfect running water. Water has no viscosity to speak of, it doesn’t foam, it doesn’t cling to the needle. A water demo tells you the machine turns on — nothing more.
So when an engineering team asks me to prove vacuum is necessary, I don’t argue. I ask them to ship us their actual gel, and we run it side by side: atmospheric fill versus vacuum fill, same pump, same syringe. The bubbles settle the argument better than I can. Insist on that test at FAT — from us or from any supplier you are evaluating.
Procurement checklist before you specify
Take these to your supplier evaluation
- Documented viscosity at fill temperature (cP) and any shear-thinning behaviour.
- Oxygen sensitivity / stability data — does headspace O₂ affect shelf life?
- Syringe format, barrel volume and stopper type (nested SCF tub reference).
- Target batch size and annual volume — drives single vs. double head.
- Required cleanroom grade and whether a Grade A LAF hood or RABS integration is needed.
- A FAT protocol that runs your product, with an agreed acceptance criterion for visible bubbles.
- Documentation scope: material certificates, FAT/IQ/OQ templates — see our IQ/OQ/PQ guide.
Frequently asked questions
At what viscosity should we switch from standard to vacuum filling?
Does vacuum filling reduce throughput?
Can vacuum filling help with oxygen-sensitive biologics?
Is a vacuum machine harder to validate?
Should we buy vacuum capability now if our current product is aqueous?
Vacuum vs. Standard Syringe Filling — Reference Facts
Specify the Right Filling Method the First Time
Send us your viscosity data, syringe format and batch size. Our engineers will tell you whether vacuum is necessary — and quote only the configuration your process actually requires.
Get Free Turnkey QuoteContinue Reading
HIJ-GZB-100 vacuum filling machine
The reference machine: 0.5–20 ml, 600–800/hr, from US$26,000 FOB.
GuideHow much a syringe filler costs
Itemised pricing from base machine to fully-configured aseptic line.
GuideVacuum vs. standard filling
Viscosity and oxygen sensitivity decide the method — not budget.
GuideSingle-head vs. double-head
A second needle gives ~1.5× throughput, not 2×. The CAPEX maths.
Continue Reading
The HIJ-GZB-100 vacuum syringe filler
Full specification, transparent pricing and configuration options.
GuideThroughput and CAPEX compared
Cost per syringe-per-hour, and the ~175,000/year break-even point.
GuideWhat extra formats really cost
Mold, valve, changeover downtime and requalification — the full stack.
GuideDocumentation your supplier must provide
FAT, IQ and OQ deliverables — and where your responsibility begins.
Continue Reading
Prefilled syringe vacuum filling machine
Vacuum fill and vacuum stopper for bubble-free, oxygen-free syringes.
GuideFilling hyaluronic acid bubble-free
Why a bubble in cross-linked gel never rises out — and what it costs.
GuideOxygen-sensitive biologics
A 0.5 mL air headspace supplies ~6.4 O₂ molecules per antibody.
GuideAdding a second filling needle
When vacuum and higher throughput are both required.
Continue Reading
Vacuum filling & stoppering machine
Servo ceramic plunger pump, ±1–2% on viscous gels.
GuideWhy vacuum, not atmospheric
The reject-cost model that settles the specification argument.
GuideHeadspace oxygen and shelf life
Oxidation, silicone oil and tungsten: the three aggregation pathways.
GuideFormat tooling for 2.25 ml and above
Nest counts, molds and the ceramic-valve sharing rule.
Continue Reading
HIJ-GZB-100 aseptic syringe filler
Vacuum stoppering — the direct lever on headspace oxygen.
GuideThe case for vacuum filling
Viscosity and oxygen sensitivity decide the fill method.
GuideIQ/OQ/PQ scope for an aseptic line
Qualify vacuum level and dwell time as process parameters.
GuideViscous gels and dermal fillers
Shear-thinning rheology and the product-loss model.
Continue Reading
A machine that runs 0.5–20 ml SCF syringes
One format mold set included; change parts per additional format.
GuideWhat a prefilled syringe filling machine is
The process, the machine types, and how to choose one.
GuideRequalifying after a format change
Which documents the supplier owes you, and which are yours.
GuideTooling costs on a double-head line
Molds cost roughly 2× more when two needle positions must be tooled.
Continue Reading
cGMP-ready HIJ-GZB-100
AISI 316L contact parts, no dead corners, full documentation package.
GuideSpecifying the fill method before DQ
Vacuum or atmospheric — a URS decision, not an afterthought.
GuideWhat to measure at FAT for biologics
Headspace gas analysis and sub-visible particle counts on your protein.
GuideValidation scope for two machines vs one
Redundancy costs a second qualification exercise.
Continue Reading
Single-needle HIJ-GZB-100
600–800 syringes/hour, from US$26,000 FOB Ningbo.
GuideWhether you need vacuum at all
Product viscosity and oxygen sensitivity decide, not throughput.
GuideChange-part costs on a double-head
Molds ~US$4,800 vs ~US$2,300; ceramic valves supplied in pairs.
GuideValidating two machines instead of one
The supplier-vs-manufacturer responsibility split.